Download Obie App
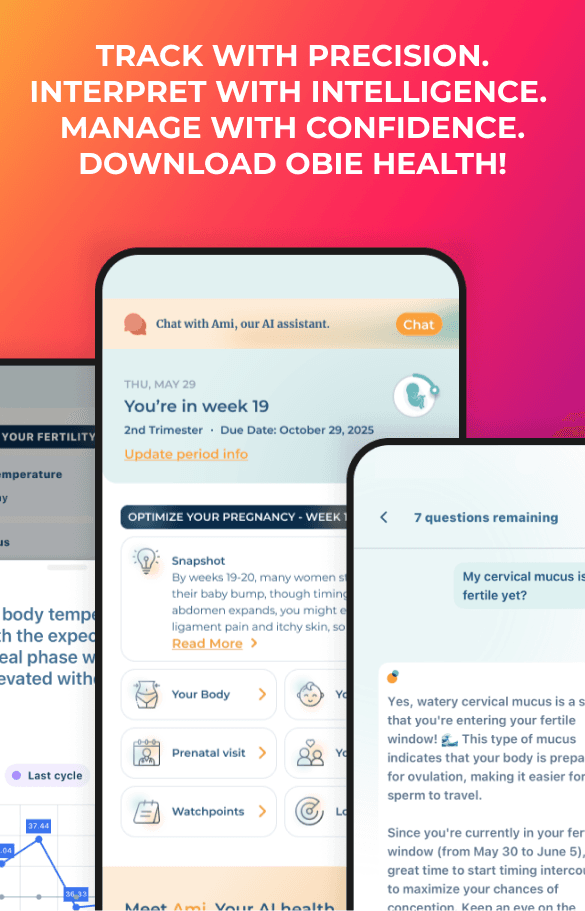
Track with precision. Interpret with intelligence. Manage with confidence.
Resources
Tools & Calculators
Obie App
Download Obie App
Track with precision. Interpret with intelligence. Manage with confidence.
App Store
Android